
Commentary: “A very unusual carotid shunt migration”
Josip Figl1*, Suzana Figl2
1Josip Figl, Department of Vascular surgery, University of Zagreb, KišpatiÄeva 12, 10000 Zagreb, Croatia, EU
2Department of plastic surgery, University of Zagreb, KišpatiÄeva 12, 10000 Zagreb, Croatia, EU
In the article “A very unusual carotid shunt migration1”, it was presented a 64 years old male patient with an extremely rare carotid shunt complication. The patient presented with a glomus tumor which encased the right carotid artery bifurcation and both internal and external carotid artery. During the tumor removal surgery, after removing the tumor, the internal carotid artery had to be reconstructed and temporary Burbank carotid shunt (Bard Peripheral Vascular, Tempe, AZ, USA) was placed. After completing the reconstruction, the shunt had to be removed, but it managed to migrate. It would be expected for a shunt to migrate downstream, towards the head, or outside the vessel, but here it somehow migrated upstream, against the blood-flow in the aortic root (Figure 1, arrowed). The details about how and the exact events around the shunt migration could not be obtained from the outside facility. The patient was hemodynamically stable, the reconstruction was finished, endovascular retrograde approach through the common carotid artery incision during surgery was not taken into consideration in this hospital and the patient was transferred urgently to our hospital where he was re-operated by the cardiac surgeon. Endovascular procedure was deemed too risky to cause more vascular or cardiac trauma. A sternotomy was done and in mild hypothermia and cardiac arrest, the aortic root was opened and the shunt was extracted. After two days, the hemodynamically stable patient was re-transferred to the hospital in which the original surgery was done.
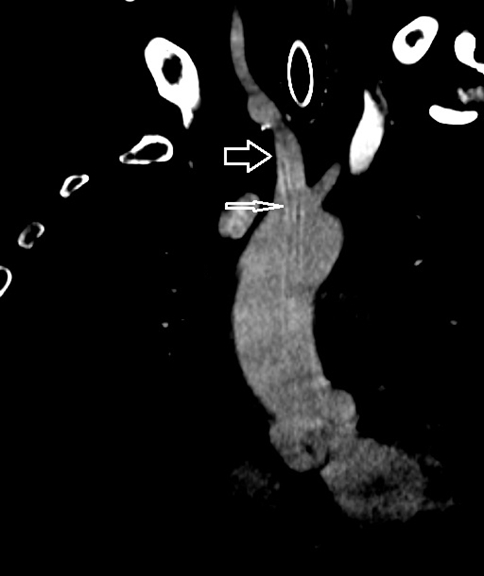
Figure 1: Thick arrow – brachiocephalic artery. Thin arrow – migrated shunt.
This is very rare and unusual carotid shunt complication. It would be normal for the blood-flow to flush the shunt towards the head or out of the artery, but in this patent it was the other way around – the shunt somehow migrated proximally, into the aortic root.
In situations like this, there is always a therapeutic question whether to extract this foreign material or to leave it with a life-long anticoagulant therapy. There is no consensus about it in literature nor in surgeons’ opinions. The negative aspect of non-extraction is life-long anticoagulant therapy with its possible complications, and the patient always has a potential embolic source, a foreign material prone to bacterial aggregation and infection. The negative aspect of the decision to extract the shunt lies in its invasiveness and all the complications related to it. For extraction, it can be used as a first line endovascular attempt, a minimally invasive technique, which usually can solve the problem via femoral access, but in this particular patient the estimated risk of further vascular trauma was too high. This led to decision for open surgical extraction. The cardiac surgeons decided to perform an urgent midline sternotomy and to extract the shunt surgically. This way, the potential embolic source was removed and potential greater vascular and cardiac damage which might occur in the future due to constant movement of the shunt was prevented.
Conflict of Interest
The author declares no conflict of interest.
References
- Figl J, Perkov D, A Very Unusual Carotid Shunt Migration. European Journal of Vascular and Endovascular Surgery. 2020 60(1): 87, https://doi.org/10.1016/j.ejvs.2020.04.030