
CT Demonstration of Massive Enteric Bleeding in A Secondary Aortoenteric Fistula
Josip Figl1*, Suzana Figl2, Tomislav MeštroviÄ1, Damir Halužan1, Dino Papeš1, Ivan Škorak1
1Josip Figl, Tomislav MeštroviÄ1, Damir Halužan1, Dino Papeš1, Ivan Škorak, Department of Vascular surgery, University hospital centre Zagreb, KišpatiÄeva 12, 10000 Zagreb, Croatia, EU
2Suzana Figl, Department of Plastic surgery, University hospital centre Zagreb, KišpatiÄeva 12, 10000 Zagreb, Croatia, EU
The critically ill female patient was presented in the emergency department hemodynamically unstable, with hematemesis and history of previous aortic reconstruction surgery due to abdominal aortic aneurysm. Esophagogastroduodenoscopy was negative for ulcer or bleeding, but multislice computed tomographic angiography (MSCTA) revealed an aortoenteric fistula (AEF). The patient was prepared for immediate surgery – aortic prosthetic graft-to-aorta anastomotic sites reconstruction and small bowel suturing. This type of surgery was chosen due to extreme hemodynamic instability of the patient, but with good one-year follow-up.
The AEF is pathological communication between the aorta and the bowel – a very rare condition, but with high mortality rate if not treated expeditiously. Patients usually have stomach pain, low blood pressure, high heart rate and some have herald bleeding1 – couple small episodes of prodromal “gastrointestinal” bleeding before a major, lethal, bleeding. Patients may (secondary AEF) or may not have previous aortic reconstruction (primary AEF). The condition is very urgent to deal with, but it is extremely difficult to prove it with any imaging or endoscopic method, unlike the upper gastrointestinal tract bleeding, which is the first differential diagnosis.
Figure 1 presents sagittal-view reconstructions which very clearly show iodine contrast transferring from the aorta directly into the bowel (arrowed) – an explicit proof of AEF as a cause of this patient’s condition.
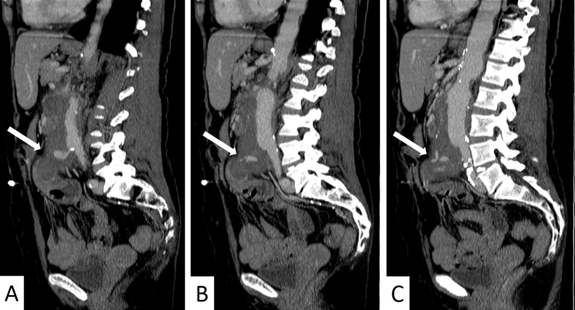
Figure 1: Aortoenteric fistula on MSCTA (sagittal view reconstructions) – iodine contrast transferring from the aorta directly into the bowel (arrowed)
Even though it usually has negative result in proving of AEFs, the computed tomographic angiography should always be performed if suspected to AEF due to necessity of aortic reconstruction. Urgent surgery is the treatment of choice, but with uncertain prognosis.
References
- Pabst TS III, Bernhard VM, McIntyre KE Sr, et al. Gastrointestinal bleeding following aortic surgery: the place of laparotomy to rule out aortoenteric fistula. J Vasc Surg. 1988; 8:280